Walk into any pharmacy and grab the cheapest magnesium bottle off the shelf. There's a roughly 80% chance you just bought magnesium oxide — the form with about a 4% absorption rate. Most women who say "magnesium didn't work for me" took the wrong form at the wrong time, and never gave the right one a chance.
The form on the label is the single biggest factor in whether magnesium does anything for your menopause symptoms. Dose matters. Timing matters. But form is the gate. Get it wrong and you mostly funded a bottle of laxative. Get it right and you have one of the best-evidenced, lowest-cost tools for menopausal sleep, anxiety, and bone density currently available.
This article covers exactly which form to buy, how much to take, when to take it, what it actually does, and — just as importantly — what it won't fix.
Why Menopause Specifically Depletes Magnesium
Most articles on magnesium and menopause skip the mechanism. They list benefits and move on. The mechanism is the part that explains why your needs change after 45, and it's worth two minutes.
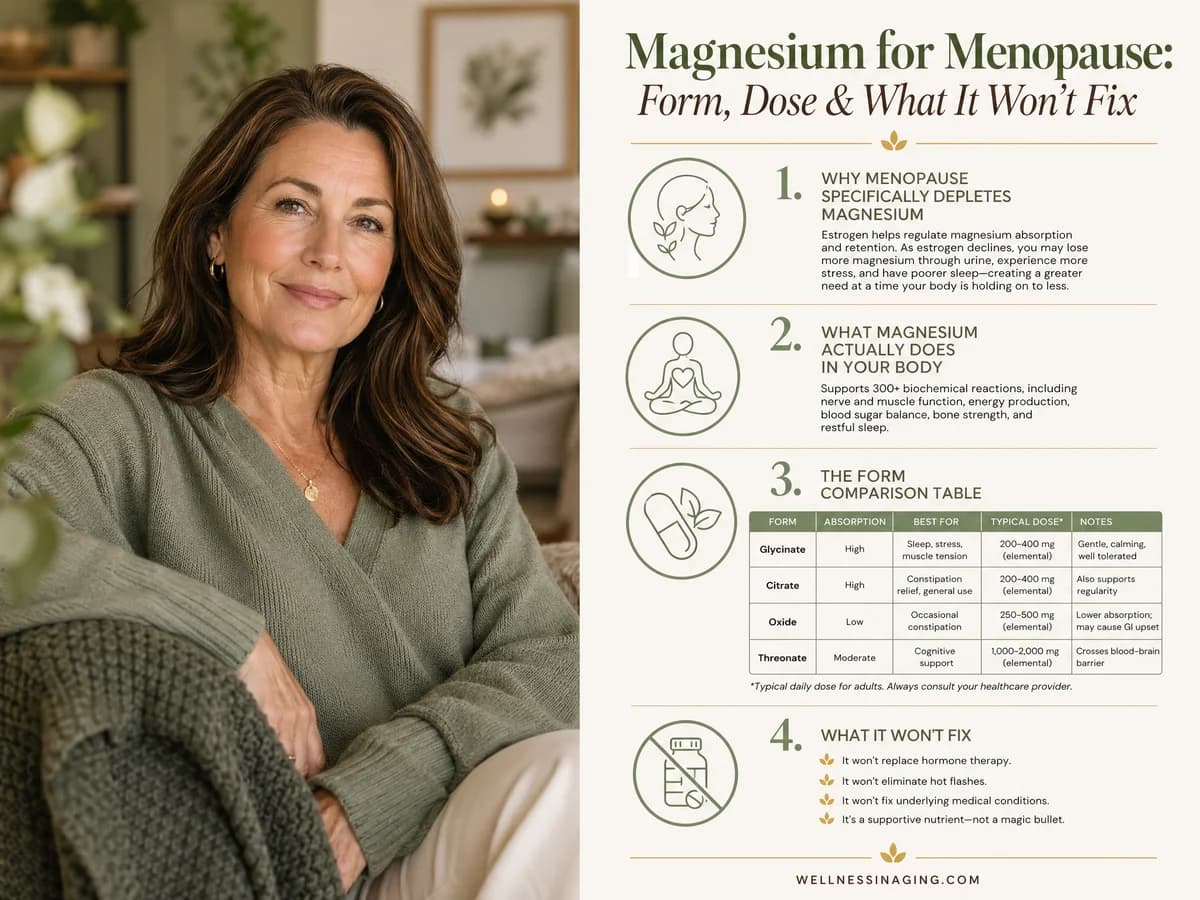
Estrogen helps your kidneys hold on to magnesium. When estrogen levels are stable, magnesium that filters through your kidneys gets reabsorbed and stays in your body. As estrogen declines through perimenopause and into postmenopause, that reabsorption weakens. More magnesium ends up in your urine. Less stays in your tissues.
A 2017 study in the Journal of Women's Health (Muñoz et al.) confirmed this with measurable data: postmenopausal women had significantly lower serum and intracellular magnesium levels than premenopausal women, and the difference tracked with the estrogen drop — not with diet, not with age alone.
Two other things compound the problem. First, intestinal magnesium absorption decreases with age regardless of hormones (Gröber et al., Nutrients, 2015). Second, the medications women in menopause commonly take — proton pump inhibitors for reflux, diuretics for blood pressure, bisphosphonates for bone density — all reduce magnesium status further.
The result: a woman who was getting by on a borderline magnesium intake at 35 can become functionally deficient at 52 without changing a single thing about her diet.
Quotable fact: Estrogen quietly does the work of helping your kidneys retain magnesium. When estrogen falls in menopause, urinary magnesium loss rises — meaning postmenopausal women need either more dietary magnesium, supplementation, or both, just to stay where they were before.
What Magnesium Actually Does in Your Body
Magnesium is a cofactor in over 300 enzymatic reactions (Volpe SL, Advances in Nutrition, 2013). The ones most relevant to menopause:
- Activates GABA receptors. GABA is the brain's primary "calm down" neurotransmitter and the system most sleep medications target. Without enough magnesium, GABA receptors don't fire efficiently.
- Regulates the HPA axis. Low magnesium amplifies cortisol release. High cortisol disrupts sleep, fuels anxiety, and contributes to the 3 a.m. wake-up so many menopausal women describe.
- Builds bone. About 26% of bone mineral content is magnesium. It also influences both osteoblast (building) and osteoclast (breakdown) activity (Rude et al., 2009).
- Activates vitamin D. This is the one almost no article mentions: vitamin D requires magnesium to convert into its active form (Uwitonze and Razzaque, JAOA, 2018). Taking vitamin D while magnesium-deficient gives you a fraction of the benefit.
- Supports muscle function. Including the smooth muscle of the gut, the skeletal muscle behind nighttime leg cramps, and the cardiac muscle behind palpitations.
That last point matters because almost every common menopause symptom — sleep problems, anxiety, joint pain, palpitations, bone loss, low vitamin D response — touches at least one of these pathways.
The Form Comparison Table
This is the table to bookmark. The supplement aisle would have you believe every form of magnesium is equally effective. The absorption data says otherwise. The form printed on the label tells you almost everything about whether this purchase will help you.
| Form | Absorption | Best For | Avoid If |
|---|---|---|---|
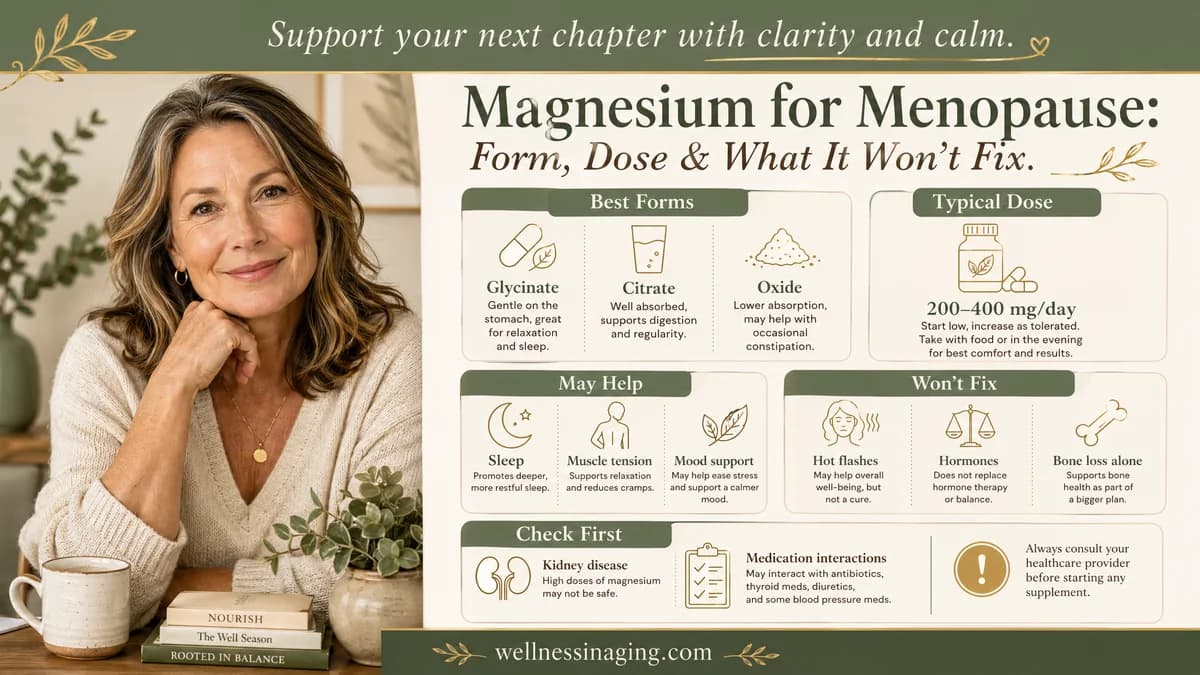
| Glycinate (or bisglycinate) | High (~46-50%) | Sleep, anxiety, general daily use, sensitive stomachs | — |
| Citrate | Moderate-High (~44%) | Constipation, general supplementation | You have IBS or get loose stools easily |
| Oxide | Low (~4%) | Not recommended for supplementation | — (this is the form to skip) |
| Malate | Moderate (~40%) | Daytime fatigue, fibromyalgia, muscle pain | Taking before bed (mildly energizing) |
| L-Threonate (Magtein) | High; brain-specific | Cognitive support, brain fog | Tight budget — it's the most expensive |
| Topical chloride (sprays/lotions) | Variable, hard to measure | GI sensitivity, supplemental route | You need a measurable dose |
A quick read of that table: glycinate is the default answer for most women in menopause. Citrate is a budget alternative if you also need help with constipation. Oxide is the form that gives magnesium a bad reputation — it's cheap because it's poorly absorbed, and the unabsorbed portion pulls water into the gut, which is why it became the go-to ingredient in laxatives.
L-threonate is the only form shown to meaningfully cross the blood-brain barrier in animal studies (Slutsky et al., Neuron, 2010). If brain fog is your dominant symptom and budget allows, it's worth considering — often stacked with glycinate at night.
The 5 Evidence-Backed Benefits for Menopause
1. Sleep Quality — Strong Evidence
The strongest evidence. Abbasi et al. (2012) ran a randomized controlled trial in elderly adults with primary insomnia: 500mg of magnesium daily for 8 weeks vs. placebo. The magnesium group fell asleep 17.78 minutes faster on average, scored significantly better on the Pittsburgh Sleep Quality Index (PSQI), had higher serum melatonin, and lower morning cortisol.
Held et al. (2002) found that 300mg of magnesium daily for 20 days increased deep (slow-wave) sleep — the restorative phase that gets squeezed in menopausal women.
What to expect: most women notice an improvement within 1 to 2 weeks. Full effect takes 4 to 8 weeks.
2. Bone Density — Moderate Evidence
Tucker et al. (1999) followed 907 elderly men and women. Those in the highest magnesium intake quartile had whole-body bone mineral density 2-3% higher than those in the lowest. Each additional 50mg of dietary magnesium per day was later linked to a 3% lower fracture risk in postmenopausal women (Ryder et al., 2005).
The mechanism: magnesium is required for parathyroid hormone function, vitamin D activation, and direct bone mineralization (Rude et al., 2009). Estrogen loss already accelerates bone breakdown after menopause; magnesium deficiency layered on top compounds the problem.
3. Anxiety and Mood — Moderate Evidence
Boyle et al. (2017) reviewed 18 studies on magnesium and anxiety in Nutrients. The pattern was consistent: supplementation produced modest but reliable reductions in subjective anxiety, with the strongest effects in people who were deficient to begin with — which describes a meaningful share of postmenopausal women.
Mechanistically, magnesium blocks NMDA receptors (a similar pathway to ketamine, much weaker), enhances GABA, and dampens HPA-axis cortisol output. For perimenopausal anxiety that didn't exist before, magnesium glycinate is one of the lower-risk first interventions worth trying.
4. Hot Flash Reduction — Limited, Indirect Evidence
This is where you need to be skeptical. The most-cited study (Shanafelt et al., 2010) used 800mg/day of magnesium oxide in breast cancer survivors experiencing chemotherapy-induced hot flashes — not naturally menopausal women. They saw roughly a 50% reduction in hot flash frequency.
Direct evidence in menopausal women is limited. Some women report fewer night flashes once their sleep stabilizes on magnesium, which may be an indirect benefit (better sleep, less waking at the onset of a flash) rather than direct vasomotor control.
The honest answer: don't buy magnesium specifically to stop hot flashes. Buy it for sleep, anxiety, and bones. If hot flashes also improve, treat that as a bonus.
5. Muscle Cramps and Joint Pain — Emerging Evidence
Less formally studied but consistently reported. Magnesium supports normal muscle relaxation. Nighttime leg cramps and the diffuse muscle aches many women develop in midlife often respond within 1 to 2 weeks of starting glycinate at 200-400mg.
Free Download: Menopause Starter Guide — Evidence-based strategies for managing symptoms, a supplement reference, and a symptom tracker to bring to your doctor.
The exact form, dose, and timing used in the clinical trials — plus a quick-reference chart on drug interactions and which symptoms to expect improvement in first. Download the Menopause Starter Guide →
Dosing Protocol: The Specific Numbers
Here's the practical playbook.
- Form: magnesium glycinate (or bisglycinate — same thing, different naming convention)
- Starting dose: 100-150mg elemental magnesium, taken 30-60 minutes before bed, for the first 5-7 days
- Titration: increase by 100mg every 5-7 days until you reach 200-400mg
- Maintenance: 200-400mg nightly
- Timing: evening for sleep benefit; split-dosed (morning + evening) if your goal is anxiety or muscle cramps during the day
- NIH supplemental upper limit: 350mg/day from supplements specifically (food-source magnesium does not count toward this)
- Time to results: sleep changes in 1-2 weeks; anxiety in 2-4 weeks; bone benefits accrue over months and are measured by DEXA, not by how you feel
A note on the 350mg supplemental UL: many clinicians consider 400mg from a well-absorbed glycinate form generally safe in healthy adults, but going higher than that without a clinician's input invites GI side effects and can be problematic if you have any kidney impairment. Stay at or near the UL unless someone tracking your labs tells you otherwise.
Quotable: The studied dose range for menopausal sleep and anxiety is 200-400mg of magnesium glycinate, taken 30-60 minutes before bed. Start at 100-150mg, build up over two weeks, and expect noticeable sleep changes within 14 days.
How to Stack Magnesium with Other Supplements
Magnesium doesn't work in isolation. Understanding how it interacts with the other supplements most menopausal women take helps you get more from all of them.
Magnesium + Vitamin D: This is the most important combination. Vitamin D is inactive until it's converted by an enzyme that requires magnesium as a cofactor. Research by Uwitonze and Razzaque (JAOA, 2018) found that vitamin D supplementation in magnesium-deficient individuals produced significantly lower 25(OH)D increases than in magnesium-sufficient individuals. Practical implication: if your vitamin D levels aren't responding to supplementation, check your magnesium status first.
Magnesium + Calcium: The ratio of calcium to magnesium intake matters. Most Western diets already oversupply calcium relative to magnesium. Adding a calcium supplement without corresponding magnesium can push this ratio further out of balance and may contribute to constipation. If you take calcium for bone health, ensure your magnesium intake is adequate — the generally recommended dietary ratio is 2:1 calcium to magnesium.
Magnesium + Black Cohosh: No known negative interaction. Both are commonly used for menopausal symptoms and can be taken together. Magnesium addresses sleep and anxiety; black cohosh targets vasomotor symptoms via a different pathway. They serve complementary roles.
Magnesium + Melatonin: Both support sleep onset via different mechanisms. Magnesium modulates GABA and cortisol; melatonin signals circadian timing. Some women find the combination useful, particularly when their primary complaint is difficulty falling asleep (not just staying asleep). Start one at a time to know which is doing what.
What Magnesium Won't Fix
Trust is built by being honest about limits. Here's where magnesium isn't the answer:
- Hot flashes directly. As noted above, the evidence is thin and indirect. If hot flashes are your main complaint, magnesium is supportive at best — not a primary tool. See hot flash treatment options for what actually works.
- Severe insomnia in isolation. Magnesium helps sleep architecture. It doesn't override late caffeine, an inconsistent schedule, untreated sleep apnea, or alcohol within 3 hours of bed.
- Clinical depression. Mild mood lift is realistic. Major depressive disorder needs a clinician.
- Significant bone loss already in progress. Magnesium supports bone health; it doesn't reverse osteoporosis on its own. Bone-loss treatment is a layered protocol involving vitamin D, calcium, weight-bearing exercise, sometimes bisphosphonates, and sometimes hormone therapy.
- Replacing a deficient diet. Spinach, pumpkin seeds, almonds, black beans, and dark chocolate are still your foundation. Supplementation fills the gap; it doesn't substitute for the foundation.
This isn't a reason to skip magnesium. It's a reason to have realistic expectations and to layer it with the right other tools.
Drug Interactions Women in Menopause Should Know
If you take any of these, talk to your pharmacist before adding magnesium — and watch the timing.
- Proton pump inhibitors (PPIs): Omeprazole, esomeprazole, pantoprazole. Long-term PPI use reduces magnesium absorption (FDA Drug Safety Communication, 2011). If you've been on a PPI for over a year, you may already be deficient — supplementing is often appropriate but worth a conversation with your prescriber.
- Bisphosphonates: Alendronate (Fosamax), risedronate, ibandronate. Magnesium binds to bisphosphonates in the gut and prevents both from absorbing well. Space them at least 2 hours apart — most clinicians suggest the bisphosphonate first thing in the morning and magnesium at night.
- Diuretics: Loop and thiazide diuretics increase urinary magnesium loss. Many women on these are subclinically deficient. Potassium-sparing diuretics (spironolactone) actually retain magnesium.
- Antibiotics: Fluoroquinolones (ciprofloxacin, levofloxacin) and tetracyclines bind to magnesium and lose effectiveness. Space at least 2 hours apart from a magnesium dose.
- Some blood pressure medications: Calcium channel blockers can interact mildly with very high magnesium doses. Therapeutic doses are generally fine.
Signs You May Be Deficient
Magnesium deficiency rarely shows up on a standard blood test until it's severe — most magnesium is intracellular, not in serum. Pattern recognition is more useful than a single lab value. Common signs:
- Muscle cramps, especially in the calves at night
- Eye twitches that come and go
- Poor or fragmented sleep, often with 3 a.m. waking
- New or worsening anxiety, particularly the "wired but tired" version
- Constipation
- Fatigue out of proportion to your sleep
- Heart palpitations, especially when lying down
- Sensitivity to loud noises or bright lights
If you have several of these, you're likely in the gray zone — not technically deficient on a serum test, but your body is functioning below where it should be. This is exactly the zone supplementation tends to help most.
How to Choose a Supplement Without Wasting Money
Five things to look for on the label:
- The form is named clearly. "Magnesium glycinate" or "magnesium bisglycinate." If the label just says "magnesium" without specifying form, it's almost always oxide.
- The elemental dose is listed. A 1,000mg "magnesium glycinate" capsule does not mean 1,000mg of usable magnesium — glycinate is a bonded compound, and the elemental magnesium is a fraction of that. Look for the elemental amount, usually 100-200mg per capsule.
- Third-party tested. Look for one of: USP Verified, NSF Certified, Informed Sport, or ConsumerLab tested. These seals mean an independent lab confirmed what's on the label is what's in the bottle, and that contamination is below safe thresholds.
- No excessive fillers. A small amount of magnesium stearate is fine; long ingredient lists of dyes and binders are a flag.
- Capsule, not gummy, for therapeutic dose. Gummies cap out at low doses (typically 50-80mg) and add sugar.
Ignore: marketing claims like "highly absorbable" without form disclosure, proprietary blends that hide the actual magnesium amount, and any product whose primary selling point is "extra strength" without telling you the elemental dose.
A brand-by-brand comparison of tested options is in the best magnesium supplement for menopause review.
Who This Is For — and Who It Is NOT For
This protocol is for you if:
- You're in perimenopause or postmenopause and have any combination of poor sleep, new anxiety, muscle cramps, or constipation
- You're on a long-term PPI, diuretic, or bisphosphonate
- You're supplementing vitamin D and want it to actually work
- Your diet is light on leafy greens, nuts, seeds, and legumes
- You want a low-cost, low-risk first intervention before exploring prescriptions
This is NOT for you if:
- You have moderate-to-severe kidney disease (eGFR under 30) — kidneys clear magnesium, and impaired clearance can cause dangerous buildup. This is the single biggest contraindication.
- You have myasthenia gravis or another neuromuscular disorder — discuss with your specialist first
- You're on lithium — magnesium can alter lithium levels
- You've had a recent heart block or significant bradycardia — clear with cardiology
- You're hoping it will replace working on sleep hygiene, stress management, or hormone therapy decisions you need to make with your clinician
Always consult your healthcare provider before starting any new supplement, especially if you take prescription medications or have a chronic condition.
The Bottom Line
If you're going to make one supplement change this week, make it a third-party-tested magnesium glycinate at the 200-400mg elemental dose range — and start at 100-150mg before bed tonight. Most women notice sleep changes within 14 days. If you see no improvement in 4 weeks at the proper dose and form, check whether you're on a medication that depletes magnesium, and consider whether your vitamin D and calcium intake needs adjustment too.
Compare specific brand options in the best magnesium supplement for menopause review. For the sleep side of this equation, insomnia during menopause covers what magnesium alone won't fix and what needs to be layered on top.
References
Muñoz N et al. (2017), Journal of Women's Health | Gröber U et al. (2015), Nutrients | Abbasi B et al. (2012), Journal of Research in Medical Sciences | Held K et al. (2002), Pharmacopsychiatry | Tucker KL et al. (1999), American Journal of Clinical Nutrition | Ryder KM et al. (2005), Journal of the American Geriatrics Society | Rude RK et al. (2009), Journal of the American College of Nutrition | Boyle NB et al. (2017), Nutrients | Shanafelt TD et al. (2010), Menopause | Uwitonze AM and Razzaque MS (2018), Journal of the American Osteopathic Association | Volpe SL (2013), Advances in Nutrition | Slutsky I et al. (2010), Neuron | FDA Drug Safety Communication on Proton Pump Inhibitors and Magnesium (2011)
Free Download
The Menopause Starter Guide
Evidence-rated strategies, a supplement reference, and a symptom tracker. 12 pages, free.
Frequently Asked Questions
Related Articles
Probiotics and Menopause: The Gut-Hormone Connection (What the Science Says)
Your gut bacteria directly regulate estrogen metabolism through the estrobolome. Here's what probiotics can and can't do for menopause — with strain-specific evidence for bone health, mood, and vaginal health.
Read article →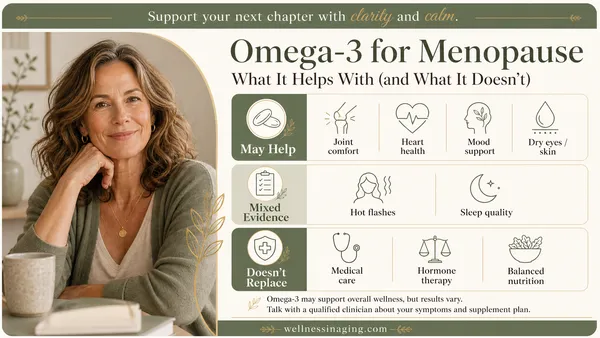
Omega-3 for Menopause: What It Helps With (and What It Doesn't)
Omega-3s have strong evidence for mood, joint pain, and heart health during menopause — but NOT for hot flashes. Here's the RCT data, the correct EPA vs DHA dose by symptom, and how to avoid rancid fish oil.
Read article →
Maca Root for Menopause: Does It Actually Work? (The Evidence)
Maca root is widely promoted for menopause. Here's what the RCTs actually show — what it helps with (libido, mood), what it doesn't (hot flashes), and the correct dose.
Read article →