Your jeans fit fine six months ago. You haven't changed what you eat. You haven't stopped exercising. And yet the number on the scale is creeping up, and the weight is settling in places it never did before — around your middle, your waist, your belly.
You're not imagining this.
Something has changed, and it's not your willpower.
This disconnect between effort and outcome is one of the most common frustrations during perimenopause and menopause. "I'm eating the same as I did five years ago and suddenly I'm gaining weight," one woman wrote on a menopause forum. "My doctor just told me to eat less and move more. That's not helpful."
She's right. It misses the mechanism entirely. Menopause changes how your body stores fat, burns energy, and responds to food. The strategies that worked at 35 often fail at 50, not because you're doing them wrong, but because your body is operating under different rules.
What follows: the specific hormonal shifts driving midlife weight gain, why standard advice often backfires, and the approaches with the strongest evidence for this phase of life.
Is this article for you? This guide is most useful if you're in perimenopause or menopause, experiencing unexplained weight gain or belly fat redistribution, and willing to prioritize strength training and protein intake over cardio and calorie restriction alone. If weight gain is sudden (10+ lbs in weeks) or accompanied by fatigue and hair loss, see your doctor first to rule out thyroid issues.
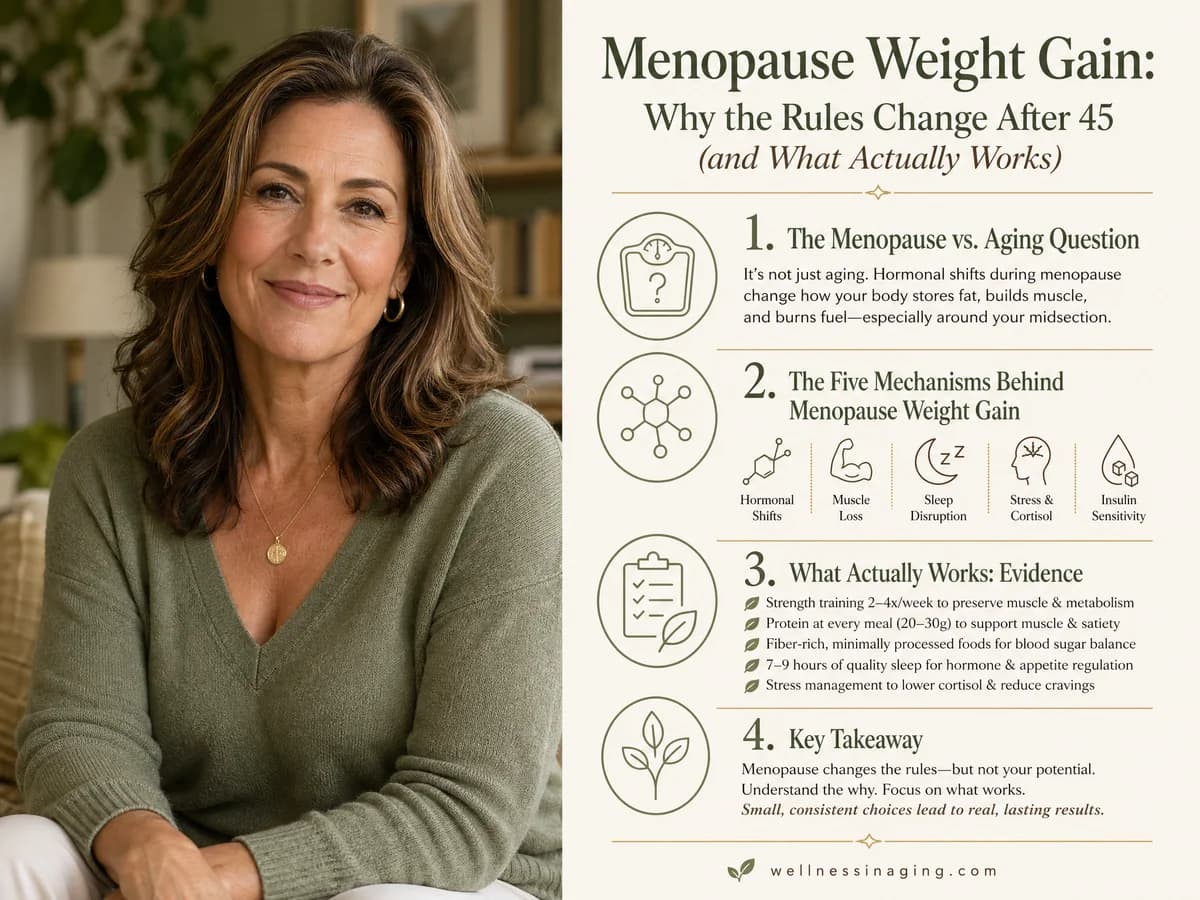
The Menopause vs. Aging Question — What the Research Actually Shows
Here's the first surprise: menopause itself doesn't cause as much weight gain as most people think. The Study of Women's Health Across the Nation (SWAN), which tracked over 3,000 women for more than a decade, found that the menopausal transition contributes only 2-5 pounds on average. The 1.5 pounds per year that most gain during midlife (ages 45-55) happens whether or not they've gone through menopause yet (Sternfeld et al., 2004).
So where does the 10-15 pounds come from? Mostly aging and lifestyle factors — declining activity, gradual muscle loss, cumulative dietary patterns. Those would happen regardless of menopause.
But here's the part that IS menopause-specific: fat redistribution.
Even if you maintain the same weight, you'll likely experience a 15-20% increase in visceral (abdominal) fat during the menopausal transition (Toth et al., 2000). The number on the scale may not change dramatically, but where the fat lives does. This is the phenomenon most women describe as feeling "different" — your waist expands even when your weight stays stable, and clothes that fit everywhere else suddenly won't button at the middle.
| What Changes | Cause | How Much |
|---|---|---|
| Total weight gain during midlife | Aging + lifestyle (not primarily menopause) | ~1.5 lbs/year, or 10-15 lbs over a decade |
| Weight gain from menopausal transition specifically | Hormonal shift | 2-5 lbs on average |
| Visceral fat increase | Estrogen decline | 15-20% increase, independent of total weight |
| Lean muscle loss | Aging + menopause combined | 5-8% reduction during the peri-menopausal window |
Source: SWAN Study; Lovejoy et al., 2008; Toth et al., 2000
The takeaway: the number on the scale is mostly aging. The belly fat is hormonal.
Understanding this distinction matters because it changes which strategies will actually work.
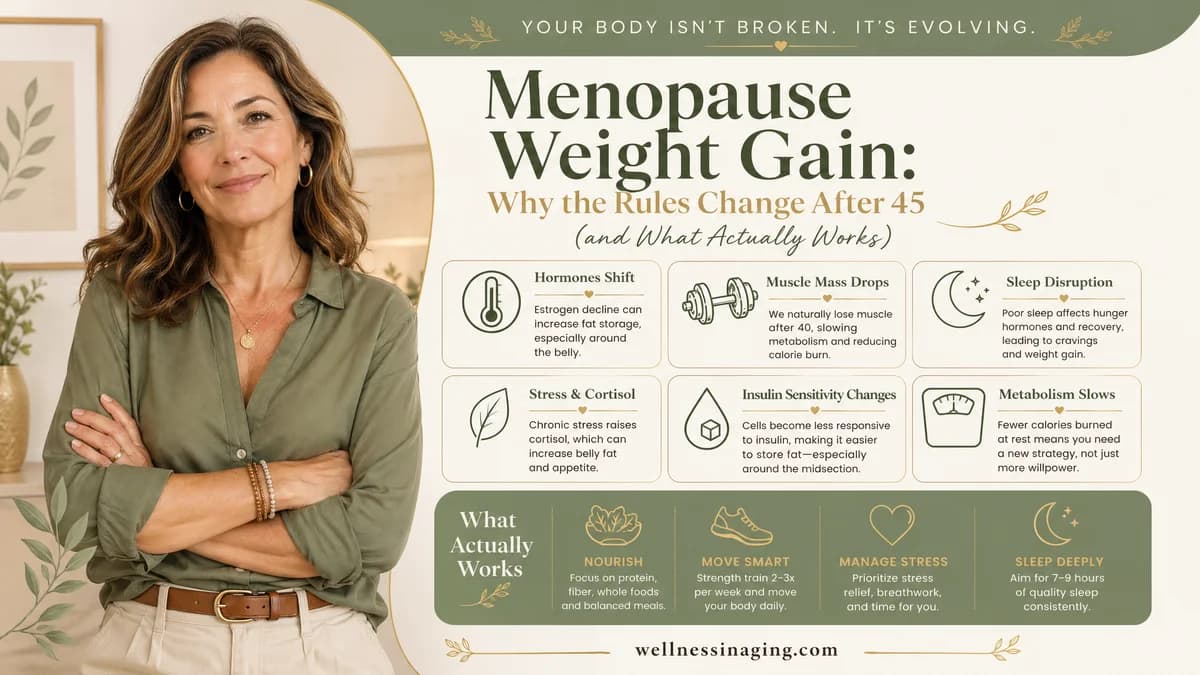
The Five Mechanisms Behind Menopause Weight Gain
Why do the rules change? Five interconnected shifts are happening in your body during perimenopause and menopause. Each one contributes to weight gain or fat redistribution, and each one requires a different response.
1. Estrogen Decline and Fat Redistribution — Moderate Evidence
Estrogen does more than regulate your cycle. It determines where your body stores fat. Before menopause, estrogen signals fat to accumulate subcutaneously — in your hips, thighs, and buttocks. When estrogen drops, that signaling disappears. Fat storage shifts to visceral depots: the abdominal cavity, around your organs, and at your waist (Lovejoy et al., 2008). This same hormonal mechanism drives hot flashes and night sweats, making vasomotor symptoms and weight changes interconnected.
This is why so many describe their body shape changing even when their weight hasn't. The fat is moving, not just accumulating.
2. Metabolic Rate Decline — Strong Evidence
Your resting metabolic rate (RMR) — the calories you burn just existing — drops by 50-70 calories per day during the menopausal transition (Poehlman et al., 1995).
That may not sound like much. Over a year, though, it adds up to 5-7 pounds if eating stays the same.
The decline comes partly from age (RMR drops 2-4% per decade after 40) and partly from muscle loss, which accelerates during menopause. Less muscle means fewer calories burned at rest.
3. Insulin Resistance — Moderate Evidence
Estrogen enhances insulin sensitivity. When estrogen falls, your cells become less responsive to insulin, meaning:
- Your muscles take up glucose less efficiently
- Your liver produces more glucose
- Your body stores more energy as fat rather than burning it
Postmenopausal women show a 20-30% reduction in insulin sensitivity compared to premenopausal women (Carr, 2003). This makes calorie restriction alone less effective — your body is more inclined to store what you eat, not burn it.
4. Sleep Disruption — Moderate Evidence
Night sweats and insomnia aren't just annoyances. Night sweats during menopause disrupt sleep architecture, raising cortisol (which promotes visceral fat storage), dysregulating hunger hormones (increasing ghrelin, decreasing leptin), and reducing the impulse control that helps you make good food choices. Those who sleep fewer than 6 hours per night gain significantly more weight over time than those who sleep 7-8 hours (Patel et al., 2008).
The sleep-weight connection is often the missing piece. I've seen countless women focus intensely on diet and exercise while running on 5 hours of fragmented sleep — and then feel completely baffled when nothing works. Poor sleep also worsens menopause brain fog, creating a cascade of cognitive and metabolic challenges.
5. Cortisol Dysregulation — Moderate Evidence
Estrogen normally buffers your stress response. Without it, your cortisol response to stress becomes exaggerated (Epel et al., 2000). Chronically elevated cortisol promotes visceral fat accumulation specifically — it's the hormone most tightly linked to belly fat.
This is why stress management isn't a luxury during menopause. It's metabolically relevant.
Free Download: Menopause Starter Guide — Evidence-based strategies for managing weight during menopause, with specific protein targets, a strength training starter plan, and a symptom tracker to bring to your doctor. Download the Menopause Starter Guide →
What Actually Works: Evidence-Ranked Strategies
Not all advice is equal. Here are the interventions with the strongest evidence for menopausal weight management, ranked by research quality.
Strength Training — Strong Evidence
This is the intervention most people underestimate or skip entirely.
Resistance training preserves lean muscle mass, which:
- Increases resting metabolic rate (1 lb of muscle burns ~6 calories per day at rest vs. 2 calories for fat)
- Improves insulin sensitivity
- Reduces visceral fat more effectively than cardio alone
In Hunter et al.'s 2000 study, postmenopausal women who did resistance training preserved their lean mass and prevented metabolic decline over one year. The control group — doing no strength training — lost muscle and gained fat despite no change in diet. A later study found that twice-weekly strength training reduced visceral fat by 8% over 16 weeks (Bea et al., 2010). For a complete guide on how to start, see strength training after 50 for women.
Specific protocol:
- Frequency: 2-3x per week minimum
- Focus: Compound movements — squats, deadlifts, rows, presses, lunges
- Intensity: Progressive overload — increase weight or reps over time
- Duration: Allow 12+ weeks to see body composition changes
The scale may not move much. Your clothes will fit differently. Muscle is denser than fat; you can weigh the same and be smaller.
Protein Intake — Strong Evidence
Protein is the most overlooked factor in midlife weight management.
It matters for three reasons:
- Thermic effect: Protein burns 20-30% of its calories during digestion (vs. 5-10% for carbs)
- Muscle preservation: Adequate protein prevents muscle loss during calorie restriction
- Satiety: Protein keeps you fuller longer, naturally reducing total calorie intake
The research is specific. Those over 50 who ate 30% of calories from protein (vs. 15%) lost more fat and preserved more muscle during weight loss (Layman et al., 2005). Distributing protein evenly — 25-30g per meal — beats eating most of it at dinner (Paddon-Jones et al., 2008).
Specific protocol:
- Target: 1.2-1.6 g protein per kg of body weight (or 0.5-0.7 g per pound)
- Distribution: 25-30g protein per meal, across 3 meals
- Timing: Protein within 1-2 hours after strength training
Example: A 150 lb (68 kg) person should aim for 80-110g protein per day. That looks like: 30g at breakfast (Greek yogurt + eggs), 30g at lunch (chicken salad), 30-40g at dinner (salmon or lean beef), with protein snacks if needed.
Sleep Quality — Moderate-Strong Evidence
Fixing sleep may do more for your weight than adjusting your diet. In Nedeltcheva et al.'s 2010 study, participants on the same calorie-restricted diet had dramatically different outcomes based on sleep: those sleeping 8.5 hours lost mostly fat (55% of total weight loss), while those sleeping 5.5 hours lost mostly muscle (only 25% of weight loss was fat).
Same diet. Different sleep. Completely different results.
Specific protocol:
- Target: 7-8 hours per night
- Address night sweats first (cooling bedding, magnesium before bed, HRT if appropriate)
- Consider CBT-I (cognitive behavioral therapy for insomnia) if sleep remains disrupted
Calorie Deficit — With Caveats — Moderate Evidence
Yes, a calorie deficit still matters. But the size of the deficit is critical during menopause, and bigger is not better.
Why aggressive deficits backfire:
- Deficits over 500 calories per day accelerate muscle loss — which is already a problem during menopause
- Muscle loss reduces metabolic rate, setting you up for rebound weight gain
- Large deficits increase cortisol, which promotes visceral fat storage
- The metabolic adaptation is disproportionate: you lose less weight than the math predicts
What works better:
- Modest deficit: 200-300 calories per day (not 500+)
- Combined with strength training to preserve muscle
- Focus on protein and fiber (not just calorie counting)
- Cyclical approach: diet breaks every 8-12 weeks to prevent metabolic adaptation
Anti-Inflammatory Diet — Moderate Evidence
The Mediterranean diet pattern improves metabolic health markers and reduces waist circumference in older adults (Estruch et al., 2013). The mechanism: reducing systemic inflammation, which links to insulin resistance and visceral fat accumulation. Following an anti-inflammatory diet during menopause addresses both weight management and symptom reduction simultaneously.
What this looks like:
- Emphasis on: vegetables, fruits, whole grains, legumes, nuts, olive oil, fish
- Limit: processed foods, refined carbs, added sugars, trans fats
- Fat isn't the enemy — quality matters more than quantity
What Does NOT Work (and Why)
Being honest about what fails builds trust and saves you time. These approaches either lack evidence or actively backfire during menopause.
Cardio-Only Exercise — Weak Evidence for Body Composition
Running, walking, cycling — these are excellent for cardiovascular health. But they don't preserve muscle mass, and they don't address the metabolic slowdown that drives midlife weight gain. In Hunter et al.'s study, aerobic exercise alone didn't prevent muscle loss or metabolic decline in postmenopausal women.
The math problem: Cardio burns calories during the workout but doesn't increase resting metabolic rate. Once the workout ends, the extra calorie burn stops. Strength training builds muscle that burns calories around the clock.
Verdict: Cardio is useful as a complement to strength training. It's not a primary tool for menopause weight management.
Aggressive Calorie Restriction — Counterproductive
Cutting 800-1,000 calories per day feels like it should work faster. It doesn't. During menopause, aggressive restriction:
- Accelerates muscle loss (up to 50% of weight lost can be muscle, not fat)
- Triggers metabolic adaptation (your body burns fewer calories than predicted)
- Raises cortisol levels (Tomiyama et al., 2010)
- Creates unsustainable misery that ends in rebound eating
Very low-calorie diets cause appetite hormone dysregulation that lasts 12+ months after the diet ends (Sumithran et al., 2011). The weight comes back, often with interest.
This is the pattern I hear constantly: "I ate 1200 calories for three months, lost 10 pounds, then gained back 15." The harder you restrict, the harder your body fights back.
Verdict: Never appropriate during menopause. A 200-300 calorie deficit with muscle preservation is sustainable; a 700-calorie deficit is metabolically destructive.
Light "Toning" Exercises with Small Weights
Three-pound dumbbells and high-rep "toning" workouts feel safer than heavy lifting. But they don't provide sufficient stimulus to build or maintain muscle. In Hunter's research, only progressive resistance training — increasing weight over time — preserved lean mass.
Verdict: If the weight feels easy by rep 12, it's too light to matter for metabolic health. Progressive overload is required.
Fat-Burner Supplements — Insufficient Evidence
Green tea extract, CLA, forskolin, garcinia cambogia — these have been studied. The results are underwhelming: 0.5-1 kg of additional weight loss over 12 weeks at best (Pittler & Ernst, 2004). Most of that is likely placebo effect.
No supplement causes meaningful weight loss without a calorie deficit and muscle preservation strategy. Some are stimulants with cardiovascular risks. None address the hormonal mechanisms driving menopausal weight gain.
Verdict: Focus on protein, strength training, and sleep. Supplements are tertiary at best.
Realistic Expectations: The Scale Is Not the Whole Story
One of the most frustrating aspects of menopausal weight management is that the scale often doesn't reflect progress.
Here's what happens when you start strength training: you may lose fat and gain muscle simultaneously. The scale stays flat or even goes up slightly. Your clothes fit better. Your waist gets smaller. You feel stronger.
But if you're only watching the number, you'll think nothing is working.
Better metrics to track:
- Waist circumference (measured at navel, first thing in morning)
- How clothes fit — especially at the waist
- Strength progression in the gym (can you lift more than last month?)
- Energy levels and sleep quality
- Fasting glucose or HbA1c if you have access to blood work
Expect body composition changes to become visible around 12 weeks of consistent strength training and adequate protein. The scale may take longer. This is normal.
A realistic outcome for a year of consistent effort: lose 5-10 lbs of fat, gain 2-4 lbs of muscle, maintain or slightly increase metabolism, reduce waist circumference by 1-3 inches. That may not sound dramatic, but it represents a meaningful health improvement — and it's sustainable.
Who This Approach Is For — and Who It Is Not
Good candidates for this approach:
- Women in perimenopause or postmenopause experiencing weight gain or fat redistribution
- Women who have tried calorie restriction alone without success
- Women willing to prioritize strength training over cardio
- Women open to tracking protein intake for 4-8 weeks to establish new habits
See your doctor first if:
- Weight gain is sudden (more than 10 lbs in a few months) and unexplained
- Weight gain is accompanied by fatigue, hair loss, or feeling cold — possible thyroid issue
- You have a history of disordered eating
- You are considering HRT and want to discuss its role in weight management
- You have joint issues that make strength training feel inaccessible (a physical therapist can modify)
The Bottom Line
Start with two changes this week: add strength training twice per week (even bodyweight exercises count to start), and track your protein intake for three days to see where you actually are versus the 25-30g per meal target. Most people are shocked by the protein gap.
If the scale hasn't budged despite consistent effort, stop watching it. Measure your waist instead. Take progress photos. Track your lifts. Body composition changes happen on a different timeline than scale weight — and they matter more for metabolic health.
Download the Menopause Starter Guide → — includes evidence-based protocols for weight management, symptom tracking, and conversation starters for your healthcare provider.
Want weekly evidence-based menopause tips delivered to your inbox? Subscribe to our newsletter at the bottom of this page.
References
- Davis, S. R., et al. (2012). Understanding weight gain at menopause. Climacteric, 15(5), 419-429.
- Lovejoy, J. C., et al. (2008). Increased visceral fat and decreased energy expenditure during the menopausal transition. Journal of Clinical Endocrinology & Metabolism, 93(5), 1772-1778.
- Sternfeld, B., et al. (2004). Physical activity and changes in weight and waist circumference in midlife women: findings from the Study of Women's Health Across the Nation. American Journal of Epidemiology, 160(9), 912-922.
- Toth, M. J., et al. (2000). Menopause-related changes in body fat distribution. American Journal of Physiology-Endocrinology and Metabolism, 279(3), E589-E600.
- Poehlman, E. T., et al. (1995). Changes in energy balance and body composition at menopause: a controlled longitudinal study. American Journal of Clinical Nutrition, 123(3), 408-415.
- Carr, M. C. (2003). The emergence of the metabolic syndrome with menopause. Endocrine Reviews, 24(1), 120-138.
- Hunter, G. R., et al. (2000). Resistance training conserves fat-free mass and resting energy expenditure following weight loss. Metabolism, 49(2), 164-170.
- Bea, J. W., et al. (2010). Resistance training predicts 6-yr body composition change in postmenopausal women. Medicine & Science in Sports & Exercise, 42(7), 1286-1295.
- Layman, D. K., et al. (2005). Dietary protein and exercise have additive effects on body composition during weight loss in adult women. Journal of Nutrition, 135(8), 1903-1910.
- Paddon-Jones, D., et al. (2008). Protein, weight management, and satiety. American Journal of Clinical Nutrition, 87(5), 1558S-1561S.
- Estruch, R., et al. (2013). Primary prevention of cardiovascular disease with a Mediterranean diet. New England Journal of Medicine, 368(14), 1279-1290.
- Epel, E., et al. (2000). Stress and body shape: stress-induced cortisol secretion is consistently greater among women with central fat. Psychosomatic Medicine, 62(5), 623-632.
- Patel, S. R., et al. (2008). Sleep duration and obesity. Obesity, 16(3), 643-653.
- Nedeltcheva, A. V., et al. (2010). Insufficient sleep undermines dietary efforts to reduce adiposity. Annals of Internal Medicine, 153(7), 435-441.
- Tomiyama, A. J., et al. (2010). Low calorie dieting increases cortisol. Psychosomatic Medicine, 72(4), 357-364.
- Sumithran, P., et al. (2011). Long-term persistence of hormonal adaptations to weight loss. New England Journal of Medicine, 365(17), 1597-1604.
- Pittler, M. H., & Ernst, E. (2004). Dietary supplements for body-weight reduction: a systematic review. International Journal of Obesity, 28(4), 509-517.
This content is for informational purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider before starting any new supplement or treatment. Individual results may vary.
Free Download
The Menopause Starter Guide
Evidence-rated strategies, a supplement reference, and a symptom tracker. 12 pages, free.
Frequently Asked Questions
Related Articles
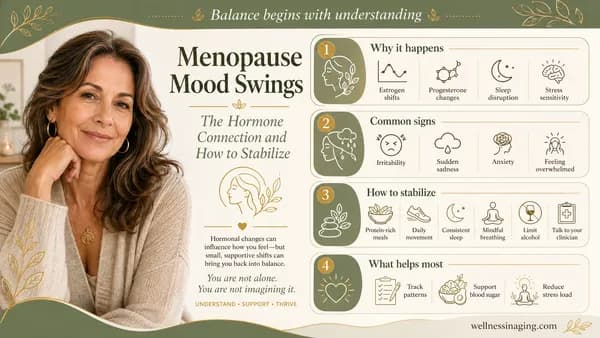
Menopause Mood Swings: The Hormone Connection and How to Stabilize
Why estrogen fluctuations cause dramatic mood changes during menopause — and evidence-based approaches from lifestyle to supplements to therapy.
Read article →
Joint Pain During Menopause: The Estrogen Connection and Natural Relief
Why declining estrogen causes joint pain during menopause — and which supplements, exercises, and lifestyle changes have clinical evidence behind them.
Read article →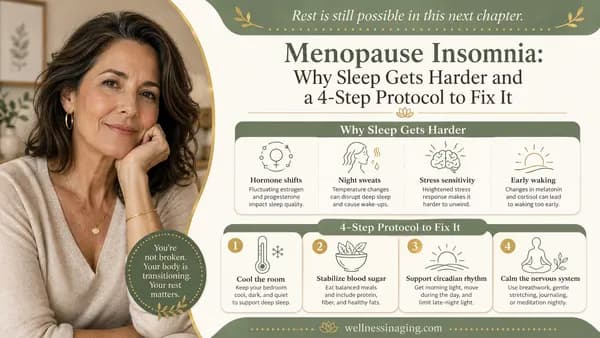
Menopause Insomnia: Why Sleep Gets Harder and a 4-Step Protocol to Fix It
Menopause disrupts sleep through four distinct mechanisms. This guide explains each one and gives you a specific, prioritized protocol to fix them.
Read article →