This content is for informational purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider before starting any new supplement or treatment. Individual results may vary.
Free Download: Menopause Starter Guide — Evidence-based strategies for managing symptoms, a supplement reference, and a symptom tracker to bring to your doctor.
Download the Menopause Starter Guide →
If you're scared you're developing dementia, take a breath. Menopause brain fog is real — it shows up on brain scans, it's documented in research, and it is absolutely not "all in your head." But it is also not Alzheimer's disease. For most women, it is temporary.
The fear itself makes it worse. When you're convinced something is seriously wrong with your brain, anxiety ramps up cortisol — which directly impairs the hippocampus, the brain region most responsible for memory. Understanding what's actually happening, and why it will likely improve, is the first useful step.
About 60% of menopausal women report subjective cognitive difficulties — memory lapses, trouble finding words, difficulty concentrating, mental fatigue (Weber et al., Journal of Steroid Biochemistry and Molecular Biology, 2013). Objective testing confirms that subtle but measurable declines in verbal memory and processing speed do occur during perimenopause. The symptoms are real. They are also typically reversible.
What's Actually Happening in Your Brain
Estrogen does far more in the brain than most people realize. Estrogen receptors are densely distributed throughout the hippocampus (memory formation), the prefrontal cortex (executive function, working memory, attention), and the amygdala (emotional processing).
When estrogen levels drop during menopause, several things happen simultaneously:
Neurotransmitter changes: Estrogen supports the production of acetylcholine, the neurotransmitter most closely associated with memory and learning. It also modulates serotonin and dopamine, which affect focus and mental clarity. When estrogen declines, cholinergic signaling weakens — memory encoding and retrieval become less efficient.
Metabolic stress in the brain: A 2017 PET imaging study by Mosconi et al. found that perimenopausal women showed a 20–30% reduction in brain glucose metabolism in the hippocampus and prefrontal cortex compared to premenopausal women. The brain runs on glucose. When its ability to use glucose drops by nearly a third during the menopause transition, mental fogginess is a predictable result.
Postmenopausal women in the same study showed partial recovery of glucose metabolism — the brain adapts to the new hormonal environment. This adaptation period is what you're living through.
Neuroinflammation: Lower estrogen is associated with increased neuroinflammation, which slows cognitive processing and contributes to mental fatigue.
Sleep deprivation: This one gets less attention than it deserves. If you're waking up two, three, or four times a night drenched in sweat, your brain fog may be primarily driven by sleep fragmentation rather than hormones directly. REM sleep is when the brain consolidates memories — transferring them from short-term to long-term storage. Interrupted REM sleep doesn't just leave you tired; it actively impairs memory consolidation the following day.
Research from Joffe et al. (2010) found that sleep quality was a stronger predictor of cognitive and mood symptoms than hot flash severity. Treating night sweats can dramatically improve "brain fog" without any direct cognitive intervention.
Brain Fog vs. Dementia: How to Tell the Difference
This is the question that keeps women up at night — and it deserves a direct answer.
| Menopause Brain Fog | Dementia / Alzheimer's | |
|---|---|---|
| Onset | Gradual, in 40s–50s, coincides with menopause | Typically after 65 (early-onset Alzheimer's is rare, under 5% of cases) |
| Pattern | Fluctuates; worse with poor sleep, high stress | Steady, progressive decline over months to years |
| What you forget | Where you put your keys, the word that's on the tip of your tongue, why you walked into a room | Entire conversations, familiar routes, how to do tasks you've done for decades |
| Daily function | Frustrating but does NOT significantly interfere with your job or household | Progressively interferes with independence |
| Insight | You are aware of and frustrated by the lapses | Often lacks awareness; family notices before the person does |
| Direction | Stabilizes or improves in postmenopause | Continuously worsens |
Red flags that warrant neurological evaluation:
- Cognitive symptoms beginning suddenly after age 60 (not the gradual onset of perimenopause)
- Progressive worsening over 6–12 months with no improvement
- Getting lost in familiar places
- Forgetting entire conversations or events — not "I forgot where I put my keys" but "I don't remember that conversation ever happened"
- Family members expressing concern before you are
- Difficulty with previously mastered skills (a lifelong accountant suddenly unable to balance a checkbook)
- Personality or behavioral changes: new apathy, suspicion, or disinhibition
If any of these apply, see your doctor. Menopause brain fog alone doesn't look like this.
How Long Does Brain Fog Last?
Individual variation is wide, but the typical pattern follows the menopause transition:
Early perimenopause: Subtle symptoms, often dismissed as stress or "getting older." Hormone fluctuations are beginning but haven't peaked.
Late perimenopause: The worst phase. Hormone levels are erratic, sleep is severely disrupted, and cognitive symptoms are most pronounced. The SWAN study (Greendale et al., Neurology, 2009) found measurable declines in processing speed and verbal memory during this period in a cohort of over 2,300 women.
Early postmenopause (0–2 years after final period): Symptoms begin to stabilize as the brain adapts to a consistently low-estrogen environment.
Late postmenopause (2–5 years after final period): Most women report meaningful improvement. The brain has completed its metabolic adaptation.
Factors that predict worse or longer symptoms: chronic sleep disruption, high stress, untreated anxiety or depression, physical inactivity, early menopause (surgical or premature), and smoking.
The research finding that offers the most reassurance: the cognitive declines measured during perimenopause are subtle (within 0.5 standard deviations in the SWAN study) and do not continue to worsen after menopause. This is adaptation, not degeneration.
What Actually Helps
1. Fix the sleep first
If you have night sweats disrupting sleep, this is the highest-leverage intervention. Every hour of fragmented sleep compounds cognitive impairment the next day. Strategies that specifically address night sweats (cooling bedding, treating vasomotor symptoms with HRT or black cohosh, bedroom temperature management) can produce dramatic improvement in brain fog without anything else changing.
See our full guide on night sweats during menopause for a complete protocol.
2. Hormone replacement therapy (HRT)
Evidence rating: MODERATE–STRONG (with important timing caveat)
Estrogen's role in cognitive function is well-established, but the evidence for HRT improving brain fog comes with a critical nuance: timing matters enormously.
Research consistently supports the "critical window hypothesis" — HRT initiated during perimenopause or within 5 years of the final menstrual period shows neutral-to-positive effects on verbal memory and cognitive function. HRT initiated 10 or more years after menopause (as studied in the Women's Health Initiative Memory Study) shows no cognitive benefit and may increase dementia risk.
If you're considering HRT for cognitive symptoms:
- Transdermal estrogen (patch or gel) is generally preferred over oral for cognitive outcomes — it provides more stable blood levels and avoids first-pass liver metabolism
- Typical dose: 0.05–0.1mg estradiol patch weekly, or 0.5–1mg estradiol gel daily
- Micronized progesterone (if you have a uterus) is preferred over synthetic progestins, which may have negative mood and cognitive effects
- Cognitive benefits typically emerge within 3–6 months
If you're in perimenopause or early postmenopause and experiencing significant brain fog alongside other symptoms, this is a conversation worth having with your doctor. The window for maximum cognitive benefit is open now — it won't stay open indefinitely.
3. Aerobic exercise
Evidence rating: STRONG
Exercise is one of the most robustly evidence-supported interventions for cognitive health at any age, and menopause is no exception.
A landmark study by Erickson et al. (2011) found that moderate aerobic exercise (walking 40 minutes, three times per week) increased hippocampal volume by 2% and improved memory scores in older adults. How it works: exercise increases brain-derived neurotrophic factor (BDNF), improves cerebral blood flow, reduces neuroinflammation, and promotes the formation of new neural connections.
Target: 150 minutes per week of moderate-intensity aerobic activity, plus two sessions of strength training. Both matter. Resistance exercise also supports cognitive function and appears to reduce long-term dementia risk.
4. Supplements with meaningful evidence
Omega-3 fatty acids (DHA specifically) Evidence rating: MODERATE
DHA (docosahexaenoic acid) is a structural component of neuronal membranes and supports synaptic plasticity — the brain's ability to form and strengthen connections. A 2010 RCT by Yurko-Mauro et al. found that 900mg DHA daily improved memory and learning in older adults with age-related cognitive decline.
- Dose: 500–1000mg DHA daily (from fish oil or algae oil). Look for third-party testing (IFOS or USP certification).
- Timeline: Allow 12+ weeks before assessing effect.
- Form: Algae-derived DHA is preferable if you're avoiding fish products.
Magnesium L-threonate Evidence rating: EMERGING (promising animal data, limited human trials)
Magnesium L-threonate (sold as Magtein) is the only form of magnesium shown to meaningfully cross the blood-brain barrier and raise brain magnesium levels. A 2010 study by Slutsky et al. in Neuron found it increased brain magnesium by 15% and improved learning and memory in animals. Human data is limited but promising.
- Dose: 1500–2000mg magnesium L-threonate daily (contains about 140mg elemental magnesium)
- Cost: More expensive than standard magnesium glycinate
- Timeline: 4–8 weeks
If you're already taking magnesium glycinate for sleep (which has stronger evidence and costs less), you don't need to switch — but magnesium L-threonate may be worth adding specifically for cognitive support.
B vitamins (B6, B12, folate) Evidence rating: MODERATE (particularly for elevated homocysteine)
B12 deficiency becomes increasingly common after 50 due to reduced stomach acid and dietary absorption. Elevated homocysteine — which B vitamins help lower — is associated with accelerated brain atrophy. A 2010 study by Smith et al. found B vitamin supplementation reduced brain atrophy by 30% in individuals with mild cognitive impairment and elevated homocysteine.
- Dose: B-complex with methylated forms: methylcobalamin (B12) 500–1000mcg, methylfolate 400–800mcg, B6 25–50mg
- Note: If you're vegetarian or vegan, B12 testing and supplementation is especially important
- Timeline: 2–4 weeks for subjective energy and focus improvement
5. What doesn't help (save your money)
Ginkgo biloba: The GEM Study (Snitz et al., JAMA, 2009) enrolled over 3,000 adults and found ginkgo biloba had no effect on cognitive decline or dementia incidence. Not recommended.
"Brain health" proprietary blends: These almost always contain multiple active ingredients at doses too low to have individual effect. Buy single-ingredient supplements where the dose matches what clinical studies used.
Phosphatidylserine: Inconsistent results across trials; weak evidence for the cognitive claims on labels.
Practical Strategies for Right Now
While your brain is adapting, here's how to reduce the daily friction of cognitive symptoms:
External memory systems: Smartphone reminders for appointments. A running list for anything you need to remember. Designated spots for your keys, phone, and glasses — always the same spot, every time.
Single-task deliberately: Menopause brain handles multitasking poorly. This isn't a character flaw; it's neurobiological. Close tabs, silence notifications, work on one thing at a time. It reduces the cognitive switching cost that depletes working memory.
Batch similar tasks: Group emails, calls, and administrative tasks together rather than scattering them throughout the day. Each context switch costs more cognitive energy than it should right now.
Work with your body clock: Many women find their sharpest hours shift during perimenopause. Notice when you're most mentally clear and protect that time for tasks requiring concentration.
Stabilize blood sugar: The brain runs on glucose and is sensitive to fluctuations. High-carbohydrate meals without protein or fat cause blood sugar swings that worsen brain fog. Pairing carbs with protein and fat slows absorption and smooths out cognitive energy.
Is This Article Right for You?
This article is for you if:
- You're experiencing memory lapses, word-finding difficulties, or trouble concentrating during perimenopause or early menopause
- You're worried these symptoms might be dementia (they're almost certainly not)
- You want to understand what's happening in your brain and what evidence-based interventions exist
- You're deciding whether to talk to your doctor about HRT for cognitive symptoms
- You want practical strategies to reduce the daily friction of brain fog
This probably isn't what you're looking for if:
- You have progressive cognitive symptoms that started after age 60 with no menopause connection
- You're forgetting entire conversations or events (not just where you put your keys) — see your doctor for neurological evaluation
- You're looking for a quick fix that works overnight — brain fog improvement takes time and usually requires addressing sleep first
The Bottom Line
Menopause brain fog is not dementia. It is not permanent for most women. It is a neurological response to a significant hormonal transition — one that shows up on PET scans, that researchers have measured in longitudinal studies, and that most women see improve once the transition is complete and the brain has adapted.
In the meantime: prioritize sleep (especially night sweats management), consider whether HRT is appropriate for you and your timeline, exercise consistently, and use external memory systems without shame. These aren't workarounds — they're evidence-based responses to a real problem.
Your brain will adapt. The research shows it.
Take Action
Track your symptoms: Download our free Menopause Starter Guide to identify patterns and determine whether sleep disruption or hormonal changes are the primary driver.
Need support now? If you're also dealing with sleep disruption, our newsletter includes weekly evidence-based tips for managing menopause symptoms — including the sleep-brain fog connection.
Related Reading
- Night Sweats During Menopause — treating night sweats often resolves brain fog
- Magnesium for Menopause — sleep support that reduces cognitive impact
- HRT vs Natural Remedies — full decision framework for the HRT question
- Anxiety During Menopause — anxiety and brain fog often coexist
References
- Weber MT, et al. (2013). "Cognition and mood in perimenopause: a systematic review and meta-analysis." Journal of Steroid Biochemistry and Molecular Biology, 142: 90–98.
- Greendale GA, et al. (2009). "Effects of the menopause transition and hormone use on cognitive performance in midlife women." Neurology, 72(21): 1850–1857.
- Mosconi L, et al. (2017). "Perimenopause and emergence of an Alzheimer's bioenergetic phenotype in brain and periphery." PLoS One, 12(10): e0185926.
- Maki PM, Sundermann E. (2009). "Hormone therapy and cognitive function." Human Reproduction Update, 15(6): 667–681.
- Joffe H, et al. (2010). "Increased estradiol and improved sleep, but not hot flashes, predict enhanced mood during the menopausal transition." Journal of Clinical Endocrinology & Metabolism, 95(3): 1199–1208.
- Erickson KI, et al. (2011). "Exercise training increases size of hippocampus and improves memory." PNAS, 108(7): 3017–3022.
- Yurko-Mauro K, et al. (2010). "Beneficial effects of docosahexaenoic acid on cognition in age-related cognitive decline." Alzheimer's & Dementia, 6(6): 456–464.
- Slutsky I, et al. (2010). "Enhancement of learning and memory by elevating brain magnesium." Neuron, 65(2): 165–177.
- Smith AD, et al. (2010). "Homocysteine-lowering by B vitamins slows the rate of accelerated brain atrophy in mild cognitive impairment." PLoS One, 5(9): e12244.
- Snitz BE, et al. (2009). "Ginkgo biloba for preventing cognitive decline in older adults." JAMA, 302(24): 2663–2670.
Free Download
The Menopause Starter Guide
Evidence-rated strategies, a supplement reference, and a symptom tracker. 12 pages, free.
Related Articles
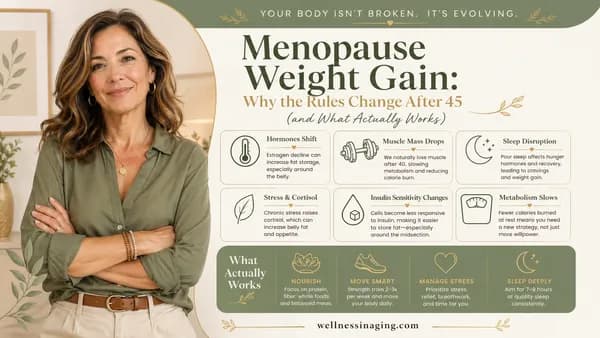
Menopause Weight Gain: Why the Rules Change After 45 (and What Actually Works)
Why menopause causes belly fat even when weight stays stable — the hormonal mechanism behind visceral fat redistribution and evidence-based strategies that work differently after 45.
Read article →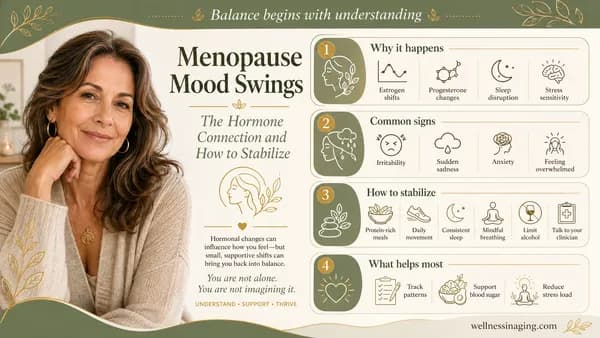
Menopause Mood Swings: The Hormone Connection and How to Stabilize
Why estrogen fluctuations cause dramatic mood changes during menopause — and evidence-based approaches from lifestyle to supplements to therapy.
Read article →
Joint Pain During Menopause: The Estrogen Connection and Natural Relief
Why declining estrogen causes joint pain during menopause — and which supplements, exercises, and lifestyle changes have clinical evidence behind them.
Read article →